NASAL CANNULA
|
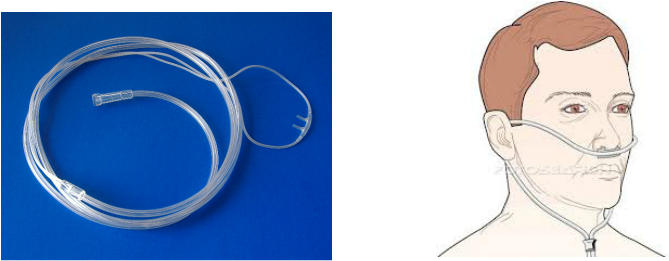
The nasal cannula (NC) is a device used to deliver supplemental oxygen or airflow to a patient or person in need of respiratory help. This device consists of a lightweight tube which on one end splits into two prongs which are placed in the nostrils and from which a mixture of air and oxygen flows.
The other end of the tube is connected to an oxygen supply such as portable oxygen generator, or a wall connection in a hospital via a flowmeter. The cannula is generally attached to the patient by way of the tube hooking around the patient's ears or by elastic head band. The earliest, and most widely used form of adult nasal cannula carries 1–6 litres of oxygen per minute. Cannulae with smaller prongs intended for infant or neonatal use can carry less than one litre per minute |
|
SIMPLE FACE MASK

The simple face mask (SFM) is a basic disposable mask, made of clear plastic, to provide oxygen therapy for patients who are experiencing conditions such as chest pain (possible heart attacks), dizziness, and minor hemorrhages. It is often set to deliver oxygen between 6-10 litres per minute. This mask is only meant for patients who are able to breathe on their own, but who may require a higher oxygen concentration than the 21% concentration found in ambient air. Patients who are unable to breathe on their own are placed on a medical ventilator instead. The final oxygen concentration delivered by a simple face mask is dependent upon the amount of room air that mixes with the oxygen the patient breathes. The air mixing is determined by how much air any individual is breathing at the moment, combined with the fit of the mask. Because of the variability in these factors, the final oxygen concentration is uncontrolled. A venturi device attached to the mask can be used to control to some degree the concentration of oxygen delivered, usually this is used to prevent respiratory depression in emphysema patients who have lost the ability to fully inhale. The effectiveness of the therapy can be continuously monitored using a pulse oximeter, though more clinically useful data can only by obtained by drawing arterial blood gas.
VENTURI MASK
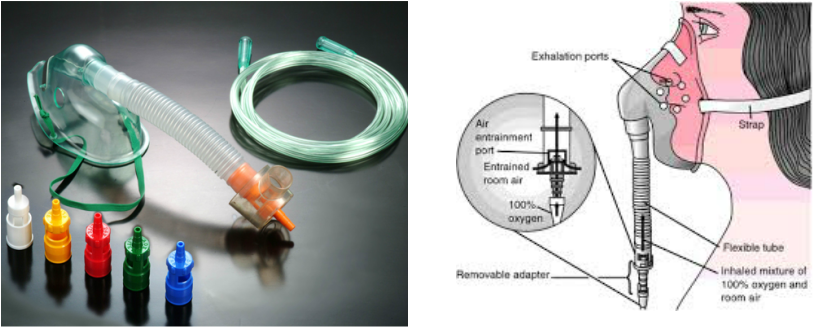
The venturi mask, also known as an air-entrainment mask (and sometimes by the brand name Ventimask®), is a medical device to deliver a known oxygen concentration to patients on controlled oxygen therapy. The mask was invented by Moran Campbell as a replacement for intermittent oxygen treatment, a practice he described as "bringing a drowning man to the surface- occasionally".Venturi masks are considered high-flow oxygen therapy devices. This is because venturi masks are able to provide total inspiratory flow at a specified FiO2 to patients therapy. The kits usually include multiple jets in order to set the desired FiO2 which are usually color-coded.Other brands of masks have a rotating attachment that controls the air entrainment window, affecting the concentration of oxygen. This system is often used with air-entrainment nebulizers to provide humidification and oxygen therapy.
NON-REBREATHER MASK (NRB)
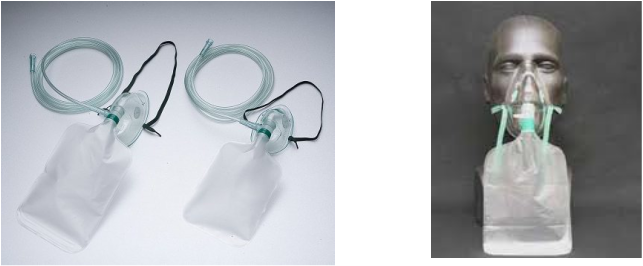
The non-rebreather mask covers both the nose and mouth of the patient and attaches with the use of an elastic cord around the patient's head. The NRB has an attached reservoir bag, typically 1 liter, that connects to an external oxygen tank or Bulk Oxygen Supply system. Before an NRB is placed on the patient, the reservoir bag is inflated to greater than two-thirds full of oxygen, at a rate of 15 liters per minute (lpm).
Approximately ¹⁄₃ of the air from the reservoir is depleted as the patient inhales, and it is then replaced by the flow from the O2 supply. If the bag becomes completely deflated, the patient will no longer have a source of air to breathe.Exhaled air is directed through a one-way valve in the mask, which prevents the inhalation of room air and the re-inhalation of exhaled air. The valve, along with a sufficient seal around the patient's nose and mouth, allows for the administration of high concentrations of oxygen, approximately 60% - 80% O2. Many textbooks report higher oxygen concentrations, however formal studies reporting these levels are not referenced to research. Please note: the patient must partially deflate the reservoir bag during inspiration or the high oxygen concentration will not be achieved, and the mask will provide only the liter flow rate setting on the flowmeter.
Ideally, a non-rebreather mask would not permit air from the surrounding environment to be inhaled. However, safety concerns regarding anti-suffocation protection in the event of a source gas failure (i.e. the oxygen cylinder allowed to drain completely) one of the two one-way valves are normally removed, allowing inhalation of outside air to a significant degree. Partial rebreather masks are designed to capture the first 150ml of the exhaled breath into the reservoir bag for inhalation during the subsequent breath. This portion of the breath was initially delivered at the end of inhalation and was therefore delivered to the "deadspace" anatomy where gas exchange did not occur. Therefore, there would be no depletion of oxygen nor gain of carbon dioxide during the rebreathing component.
Approximately ¹⁄₃ of the air from the reservoir is depleted as the patient inhales, and it is then replaced by the flow from the O2 supply. If the bag becomes completely deflated, the patient will no longer have a source of air to breathe.Exhaled air is directed through a one-way valve in the mask, which prevents the inhalation of room air and the re-inhalation of exhaled air. The valve, along with a sufficient seal around the patient's nose and mouth, allows for the administration of high concentrations of oxygen, approximately 60% - 80% O2. Many textbooks report higher oxygen concentrations, however formal studies reporting these levels are not referenced to research. Please note: the patient must partially deflate the reservoir bag during inspiration or the high oxygen concentration will not be achieved, and the mask will provide only the liter flow rate setting on the flowmeter.
Ideally, a non-rebreather mask would not permit air from the surrounding environment to be inhaled. However, safety concerns regarding anti-suffocation protection in the event of a source gas failure (i.e. the oxygen cylinder allowed to drain completely) one of the two one-way valves are normally removed, allowing inhalation of outside air to a significant degree. Partial rebreather masks are designed to capture the first 150ml of the exhaled breath into the reservoir bag for inhalation during the subsequent breath. This portion of the breath was initially delivered at the end of inhalation and was therefore delivered to the "deadspace" anatomy where gas exchange did not occur. Therefore, there would be no depletion of oxygen nor gain of carbon dioxide during the rebreathing component.
